What I Wish I'd Known When My Baby Was Diagnosed
After I delivered my son, my mind raced with questions. What now? How? Where can I find more information? What does this all mean?
The surgeons and nurses answered the questions I thought to ask... but there was so much more I didn't KNOW to ask. My surgeon told me upon first meeting him, "We are going to be around for the rest of his life! You will see me regularly until he's an adult." I love my surgeon, but here's some of the things I wish I'd been told right away and some of the most helpful things I was told (Note: My son is still a baby... we have a long way to go in this learning process.):
The surgeons and nurses answered the questions I thought to ask... but there was so much more I didn't KNOW to ask. My surgeon told me upon first meeting him, "We are going to be around for the rest of his life! You will see me regularly until he's an adult." I love my surgeon, but here's some of the things I wish I'd been told right away and some of the most helpful things I was told (Note: My son is still a baby... we have a long way to go in this learning process.):
- You are not alone. Imperforate Anus occurs 1 in 5,000 births. Anorectal malformations affect all racial, social, cultural and economic groups equally. Studies have not found any definite causes for these birth defects, which are thought to
develop during the 4th to 12th week of gestation.There are many support resources available including other parents experiencing this. - Your IA baby can live a full life. More than likely, they do not have any cognitive impairments and IA issues can be managed discreetly.
- An ostomy nurse is available to help you learn how to change bags, find the right supplies, and answer questions about the stoma.
- The stoma might change colors!!! I panicked the first time my son's stoma faded from cherry red to pale "skin color" pink. The color returned within 30 seconds, but it was very frightening to watch. As long as the stoma does not turn dark colors (grey, blue, black, purple) and the pink/red returns within one minute... it should be fine.
- The mucus fistula might change shape and size as your baby grows. My son's muscus fistula stoma started equal in size to the main stoma, then over time, shrank to be level with his skin and much smaller in diameter. My surgeon says this is fine.
- Your primary doctor or pediatrician probably has no clue how to assist with IA and doesn't know what VACTERL is. Since IA effects kids in so many different ways with high-lesion, low-lesion, fistulas and other urinary/bladder/kidney defects, your pediatrician probably doesn't fully understand the problem. Awareness about VACTERL hasn't reached the general health population. You will have to educate your doctor.
- Your child will likely need care or follow-up throughout childhood and as an adult. A nurse, doctor or consultant will help diagnose future issues with bowel management since most kids born with IA may have problems with incontinence, constipation, loose stools or other bowel concerns. These may be managed by diet, laxatives, enemas or a combination that suits your child. Most children are able to achieve voluntary bowel movements with a bowel management program. This means that they can attend school and usually participate in sports and other activities normally.
- If you qualify for government programs such as WIC, you may also be eligible for assistance for travel or other medically related needs (special foods for diet, etc.). Ask to speak to a social worker at the hospital where your child is receiving treatment.
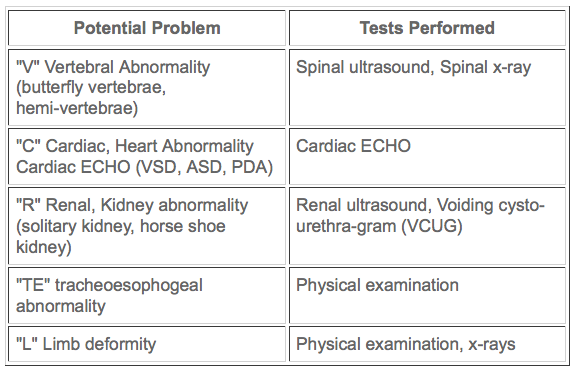
Imperforate Anus Associated Anomolies (VACTERL) & Defects
Defects of the urinary tract are the most common, and may require immediate attention. About one half of the children with an imperforate anus have other associated medical problems. Once the diagnosis of imperforate anus is made, other tests are done to look for these problems. They often use the term "VACTERL work up" to identify some of the medical problems they are looking for. "A" is for "anus" and the child has "imperforate anus". Upon completion of these tests the physician will make the diagnosis. The anatomy may be very complex in children with imperforate anus. The severity of these defects vary and your baby will be investigated for these defects. If present they will be treated as required.
This information is provided by the University of Michigan Department of Surgery, Section of Pediatric Surgery and is not intended to replace the medical advice of your doctor or health care provider. Please consult your health care provider for advice about a specific medical condition.
What is a Distal Colostogram?
From www.starship.org.nz
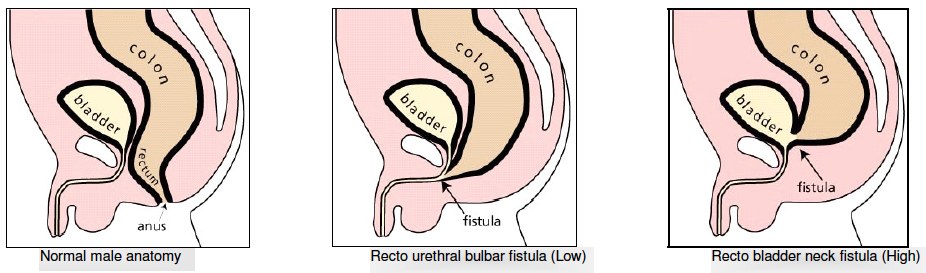
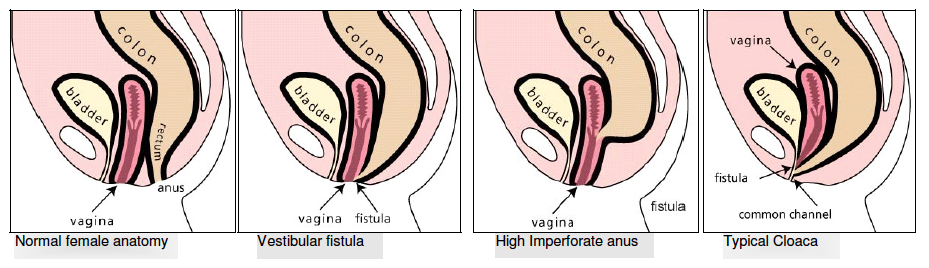
Prior to the pull-through operation (main repair), it is important to determine the precise defect your baby was born with. This will help in terms of prognostic and therapeutic implications, as well as helping the surgeon to visualise the baby’s anatomy. The distal colostogram is the best study for this, and it consists of injecting contrast material into the distal stoma (closest to the anus) to show the characteristics of the baby’s specific defect. This will show the surgeon how high the rectum is and if there is a fistula connecting to the
urinary tract.
Prior to the pull-through operation (main repair), it is important to determine the precise defect your baby was born with. This will help in terms of prognostic and therapeutic implications, as well as helping the surgeon to visualise the baby’s anatomy. The distal colostogram is the best study for this, and it consists of injecting contrast material into the distal stoma (closest to the anus) to show the characteristics of the baby’s specific defect. This will show the surgeon how high the rectum is and if there is a fistula connecting to the
urinary tract.
What is a Urodynamic Study?
The aim of the study is to provide information on your child’s bladder function which may help your child’s doctor manage your child’s urinary problems. During the study the bladder and kidney areas are screened to look for vesico-ureteric reflux (VUR).
